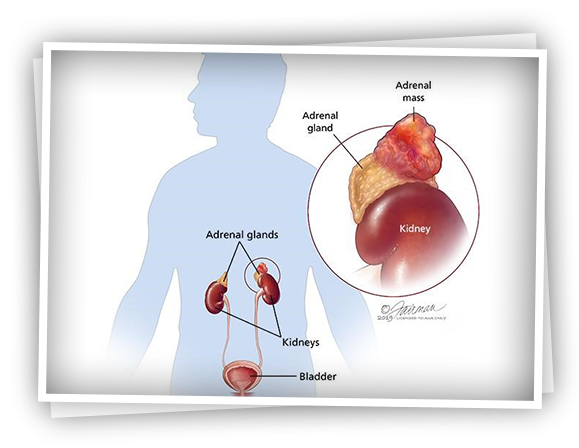
Böbrek üstü tümörlerinin teşhisi görüntüleme yöntemleri olan tomografi veya MR ile konulur. Ancak böbrek üstü bezi hormon üreten bir organ olduğu için tümörlerin de hormon üretip üretmediği incelenmelidir.
Özellikle feokromasitoma denilen böbrek üstü bezinin medullasından köken alan tümörlerde adrenalin denilen hormon kanda ve idrarda atık ürünleri yükselmiştir. Kan ve idrarda hormon seviyeleri araştırılarak tümörün hangi hormon ürettiği araştırılır.
Adrenal tumors (adenomas) smaller than 4 cm that do not produce hormones, do not cause any complaints, and are detected incidentally on imaging can be followed. If these adenomas become larger than 5 cm, they can be removed by laparoscopic surgery.
Adrenal tumors that produce hormones and cause complaints in the patient can also be treated with laparoscopic surgery.
Masses showing signs of cancer on imaging (tomography or MRI) should be removed. Hormone-producing tumors should be evaluated in detail by an endocrinologist before the surgery and the surgery should be planned after the treatment is started. The anesthesiologist should also be informed in detail about this and preparation should be made in advance.
Adenoma: Benign, non-carcinogenic tumors of the adrenal gland are called adenomas.
Small adenomas that do not produce hormones are usually followed. Adenomas that produce the hormone aldosterone are called aldosteronomas. Adenomas that produce the hormone cortisol cause Cushing's syndrome, which is characterized by weight gain, diabetes, high blood pressure, and purple lines on the abdomen.
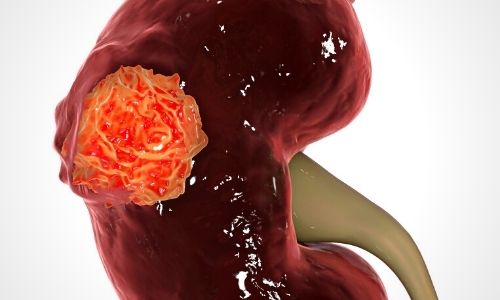
Adrenocortical carcinoma: It is a malignant, carcinogenic tumor of the adrenal gland. It is much more rare. It can be hormonally active or inactive.
Neuroblastoma: It is a tumor arising from the medulla of the adrenal gland seen in childhood.
Pheochromocytoma: It is a hormonally active tumor originating from the adrenal medulla. It progresses with high blood pressure, palpitations, sweating.
You can contact us for appointment and information.